Lifespan and Clinical Biomechanics
We do
- Investigating aging, mild cognitive impairment, and neurodegenerative diseases, and uncovering how cognitive decline alters balance and motor-control strategies.
- Advancing pediatric biomechanics through studies on cerebral palsy (CP), developmental dysplasia of the hip (DDH), and Duchenne muscular dystrophy (DMD), yielding quantitative indicators for early diagnosis and intervention.
Journal Publication
[1] Wang, J.-Y., Lu, S.-H., Hu, C.-H., Wu, K.-W., Wang, T.-M., and Lu, T.-W.*(2025). Uphill walking unveils hidden instability and biomechanical adaptations in anterior cruciate ligament-deficient copers. Gait & Posture, 120: 110008. (SCI)
[2] Chang, C.-F., Lu, T.-W., Hu, C.-H., Wu, K.-W., Kuo, C.-C., and Wang, T.-M.* (2025). Lower limb inter-joint coordination and end-point control during gait in adolescents with early treated unilateral developmental dysplasia of the hip. Bioengineering, 12(8): 836. (SCI)
[3] Lu, S.-H., Kuan, Y.-C., Wu, K.-W., Wang, T.-M., and Lu, T.-W.* (2025). Cognitive-motor dual task induces strategic kinematic adjustments with increased toe-obstacle clearance for older adults during obstacle crossing. PLOS ONE. (SCI)
[4] Lu, Y.-L., Yu, C.-H., Wang, T.-M., & Lu, T.-W.* (2025). Immediate effects of monocular viewing on lower-limb joint and endpoint kinematics during obstructed gait in young and older adults. Gait & Posture. (SCI)
Projects
Development of a Tablet-Based System for Testing and Measuring Whole-Body Balance and Endpoint Precision Control During Motor and Cognitive Dual Tasks: Effects of Cognitive Challenges in Older Adults with Cognitive Impairment of Different Severity (NSTC 2024-2027)


Figure 1. Schematic diagram showing a stick figure of a typical participant during level walking showing the COM and COP, and the COM-COP vector forming the sagittal inclination angle (IA) (A) and frontal IA (B) with the vertical. The reference limb is shown in darker grey.

Figure 2. Mean curves of the COM-COP inclination angles (IA) and their rates of change (RCIA) in the sagittal and frontal planes for the knee osteoarthritis groups 3 months after TKA via LPPA (red lines) and MVA (blue lines), and the control group (black dashed lines) during level walking in the sagittal (A, B) and frontal (C, D) planes. Positive sagittal and frontal IA indicate COM positions that are anterior and contralateral to the COP, respectively. Positive sagittal and frontal RCIA indicate rates of anterior changes and contralateral changes in the corresponding IA, respectively. Heel-strike (HS), contralateral toe-off (CTO), contralateral heel-strike (CHS) and toe-off (TO) are indicated by vertical lines. IA and RCIA were temporally normalized by the stride time to be in 0%–100% of the gait cycle. Asterisks (*) indicate statistical significance (p < 0.05) between LPPA and Control, and crosses (†) indicate statistical significance (p < 0.05) between MVA and Control for the time-averaged IA or RCIA values over double-limb support (DLS) or single limb-support (SLS) phases.
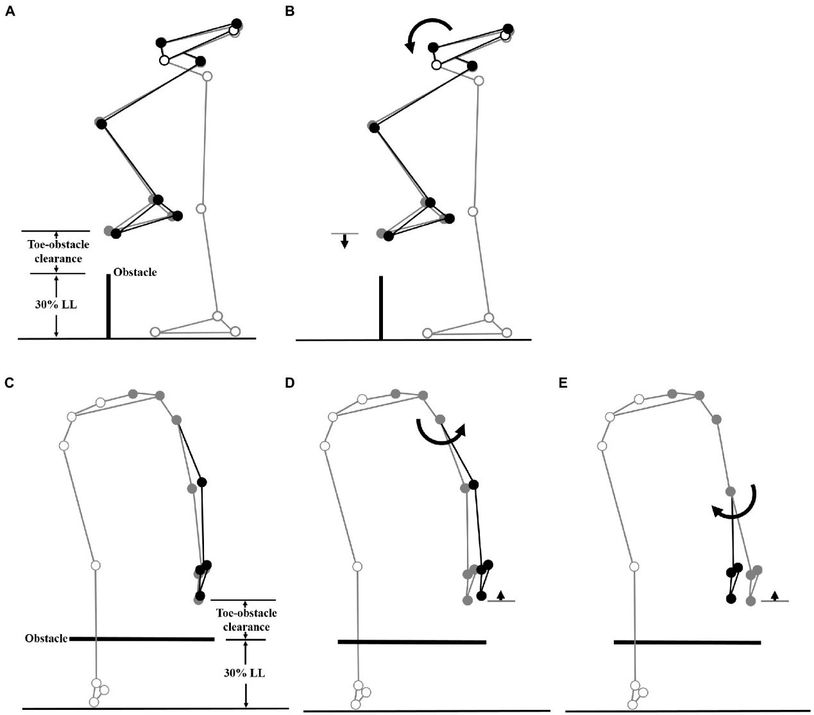
Figure 3. The planar seven-link model of the body during obstacle-crossing. Two forceplates are placed on either side of the obstacle. a Definitions of the toe-obstacle clearance and the joint angles are also indicated: hip (θ_LH), knee (θ_LK) and ankle (θ_LA) of the leading swing-limb, and foot (θ_TF), ankle (θ_TA), knee (θ_TK) and hip (θ_TH) of the trailing stance-limb. The upper body, namely the segments of the head/neck, trunk, pelvis, and upper extremities, was modeled as a single link, defined as the line connecting the hip joint center and the center of mass of all the upper body segments. The hip angles were defined as the angles between the upper body link and the thigh links. The X-axis indicates the direction of progression.
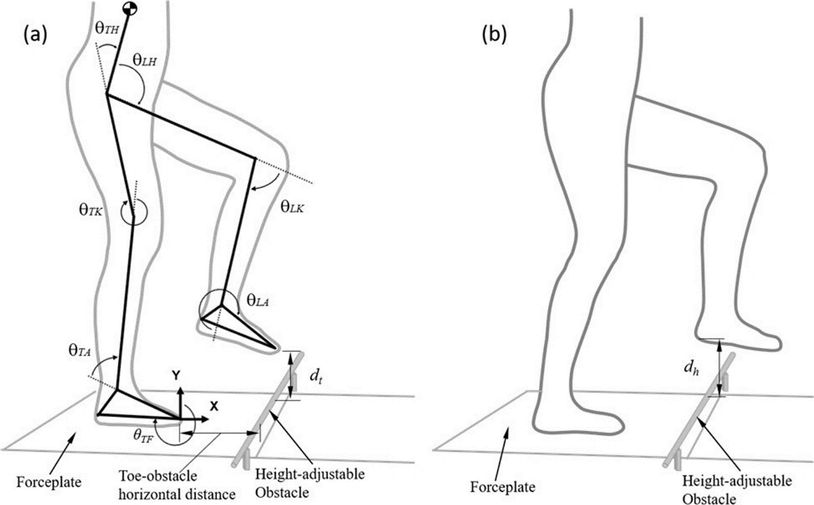
Figure 4. Effects of the observed significant angular changes at individual joints on the leading toe-obstacle clearance in the MCI group (black stick figure) compared to Control (A and C, grey stick figure) when the leading toe was above an obstacle of 30% leg length in height. The stick model was drawn using marker positions of a typical subject from each group. The segments with solid grey circles are joints of the reference limb. With the stance foot fixed to the ground, only one joint was rotated at a time, while keeping the angles of the other joints fixed, and the segments of the stance limb and the segments of the swing limb distal to the current joint stationary. The MCI group showed increased pelvic anterior tilt (B), and increased hip abduction (D) and knee adduction (E) in the swing limb. As indicated by the black stick figure, while (D, E) tended to increase the leading toe-obstacle clearance, (B) gave the opposite effect, leading to the observed normal toe-obstacle clearance.